CASE: TUBERCULOSIS
INTRODUCTORY VIDEO:
PATIENT HISTORY PRESENTATION:
 A 62-year-old man is brought to the clinic for a 3-month history of
A 62-year-old man is brought to the clinic for a 3-month history ofunintentional weight loss (12 lb). His appetite has diminished, but he
reports no vomiting or diarrhea. He does report some depressive symptoms
since the death of his wife a year ago, at which time he moved from
Hong Kong to the United States to live with his daughter. He denies a
smoking history. He complains of a 3-month history of productive cough
with greenish sputum. He has not felt feverish. He takes no medications
regularly. On examination, his temperature is 100.4°F and respiratory
rate 16 breaths per minute. His neck has a normal thyroid gland and no
cervical or supraclavicular lymphadenopathy. His chest has few scattered
rales in the left mid-lung fields and a faint expiratory wheeze on
the right. His heart rhythm is regular with no gallops or murmurs. His
 abdominal examination is benign, his rectal examination shows no
abdominal examination is benign, his rectal examination shows nomasses, and his stool is negative for occult blood. His chest X-ray is
shown in.FIGURE: COLOR CXR
➤ What is the most likely diagnosis?
➤ What is your next step?
ANSWERS TO CASE:
Summary: A 62-year-old man from Hong Kong has a 12-lb unintentional
weight loss with diminished appetite but no vomiting or diarrhea. On examination,
he has a low-grade fever, and there are a few scattered rales in the left
mid-lung fields and a faint expiratory wheeze on the right. His chest X-ray
shows a cavitary lesion (left lower lobe).
➤ Most likely diagnosis: Pulmonary tuberculosis (TB).
➤ Next step: Refer him to the hospital for admission so that serial sputum
samples can be collected for identification of the organism, and for culture
and sensitivities to guide antimicrobial therapy.

ANALYSIS
Objectives
1. Know the natural history and the clinical and radiographic manifestations
of primary and reactivation pulmonary TB and of latent TB infection.
2. Understand the methods of diagnosis of TB.
3. Learn treatment strategies for TB.
4. Know the common extrapulmonary sites of TB, including pleurisy, lymphadenitis,
miliary, meningeal, genitourinary, skeletal, and adrenal TB.
Considerations
This elderly Asian gentleman has symptoms suggestive of TB, such as weight
loss and productive cough. A chest radiograph is essential in helping to establish
the diagnosis. His chest X-ray is highly suggestive of TB, but many other
diseases may cause cavitary lung lesions, including other infections and malignancies.
If the sputum samples do not reveal acid-fast organisms, then further
testing, such as bronchoscopy, may be needed to rule out malignancy.
APPROACH TO
Suspected Tuberculosis
ALGORITHM OF TB: VIDEO
DEFINITIONS
LATENT TUBERCULOSIS: Asymptomatic infection of Mycobacterium
tuberculosis.
PRIMARY TUBERCULOSIS: Development of clinical illness immediately
after infection with M tuberculosis.
becomes active and infectious after a period of dormancy, such as years after the
initial infection.
CLINICAL APPROACH
Pulmonary Tuberculosis

Tuberculosis is a bacterial infection caused by the acid fast bacillus (AFB) M
tuberculosis, which usually is transmitted through airborne spread of droplets
from infected patients with pulmonary TB. The vast majority of cases occur
in developing countries, but a resurgence of cases in the United States
occurred during the mid-1980s as a consequence of various factors, including
human immunodeficiency virus (HIV) infection. Untreated disease can have
a 1-year mortality rate of 33% and a 5-year mortality rate as high as 50%.
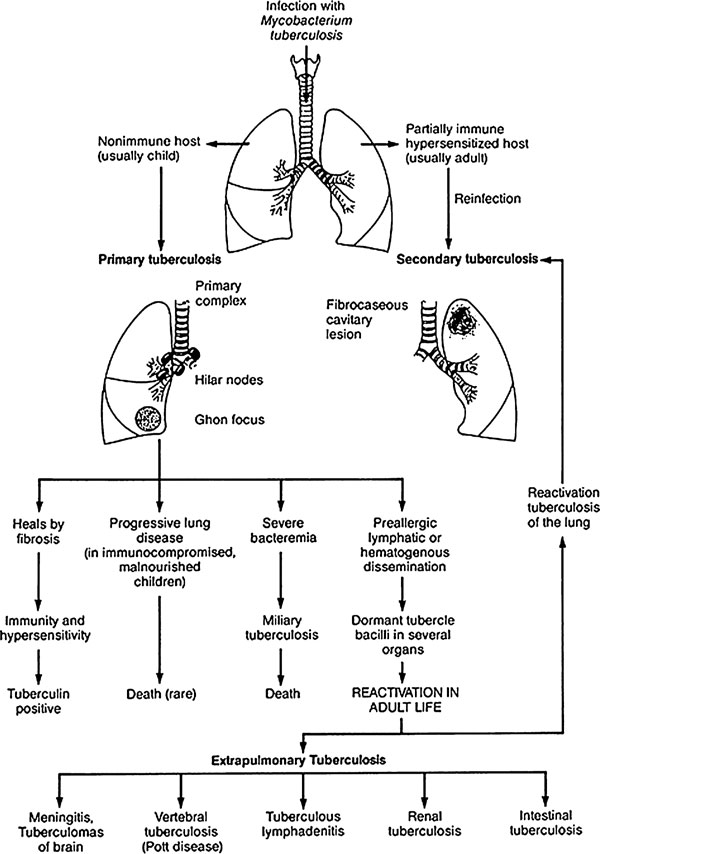
Often seen in children, primary pulmonary TB usually affects the middle
and lower lung zones. Lesions form in the periphery with hilar and paratracheal
lymphadenopathy. Granulomatous lesions are caused by the inflammatory
response of lymphocytes and macrophages. The center of the lesion may
become necrotic (caseous necrosis) and liquefied, forming a cavity. Healed
lesions are called Ghon lesions. Most patients exposed to M tuberculosis do not
manifest clinical symptoms, but they may have a latent infection. Years later,
frequently during times of stress or immunosuppression, TB may reactivate and
become symptomatic. Reactivation TB usually involves the apical and posterior
segments of the upper lobes or the superior segments of the lower lobes of
the lungs. The course may be rapid (weeks to months), chronic and slowly progressive
Signs and symptoms are nonspecific and subacute, including fever, night
sweats, malaise, weight loss, and anorexia. The cough usually is productive
of purulent sputum and sometimes streaked with blood. A lesion may erode
into a vessel, causing massive hemoptysis. Rasmussen aneurysm is the rupture
of a dilated vessel in a cavity. Physical findings can include fever, wasting,
rales and rhonchi (if there is a partial bronchial obstruction), pallor, or
finger clubbing from hypoxia. Possible laboratory abnormalities are leukocytosis,
anemia, and hyponatremia secondary to the syndrome of inappropriate
secretion of antidiuretic hormone (SIADH).
Extrapulmonary Tuberculosis
The sites, in order of decreasing frequency of occurrence, are the lymph
nodes, pleura, genitourinary tract, bones and joints, meninges, and peritoneum.
Tuberculosis lymphadenitis is common in HIV-infected patients,
children, and nonwhite women and generally is painless adenopathy. Pleural
disease can have an exudative effusion but may require pleural biopsy for diagnosis.
Tuberculosis meningitis usually has cerebrospinal fluid with high protein,
a lymphocyte predominance (or neutrophils in early infection), and low
glucose level. Adjunctive glucocorticoids may improve the treatment
response in TB meningitis. Genitourinary TB can be asymptomatic or have
local symptoms such as dysuria, hematuria, and urinary frequency. It is characterized
by the finding of leukocytes in the urine but negative bacterial cultures—
“sterile pyuria.” Skeletal TB affects weight-bearing joints, whereas Pott
disease involves the spine. Miliary TB occurs by hematogenous dissemination
with 1- to 2-mm granulomas that resemble millet seeds (hence the
name). Adrenal TB can present as adrenal insufficiency.
Diagnosis:DX
The diagnosis of TB is made by combining the history and clinical picture with
AFB stains or culture of a specimen (smear or tissue biopsy).
When pulmonary
TB is suspected, three samples of early morning sputum should be obtained
while the patient is in isolation.
Biopsy material should not be put in formaldehyde.
Cultures may take from 4 to 8 weeks on ordinary solid media or 2 to
3 weeks on liquid media.
Tuberculosis cases should be reported to the local
public health department.
Purified protein derivative (PPD) skin testing:
It is useful for screening for latent infection but has a limited role in diagnosing active
infection because of frequent false-negative results in this setting.
A positive PPD is defined by induration after 48 to 72 hours that is 5 mm or greater in
patients with HIV, close contacts of patients with TB, or patients with chest
X-ray findings consistent with TB.
People with other risk factors, such ashealth-care workers and patients who are immunocompromised for reasonsother than HIV, are considered to have a latent infection if the PPD is 10 mm
or more.
Everyone else should have less than 15 mm of induration.
...................................................................................................................................................................
PPD SKIN TEST CONFIRMATION IS DETAILED HERE; ALSO SEE LATTER IN THE CLINICAL MICROBIOLOGY SECTION BELOW FOLLOWING THIS:
Skin Testing is performed as the tuberculin or Mantoux test. PPD (purified protein derivative) is employed as the test antigen in the Mantoux test. PPD is generated by boiling a culture of MTB, specifically Old Tuberculin (OT). 5 TU (tuberculin units), which equals 0.000lmg of PPD, in a 0.1 ml volume is intracutaneously injected in the forearm. The test is read within 48-72 hours.

Administering the Mantoux test. CDC.
BELOW IS THE VIDEO STREAMING TO DEMONSTRATE HOW PPD skin test is done:
The test is considered
1. Positive test
if the diameter of the resulting lesion is 10 mm or greater. The lesion is characterized by erythema (redness) and swelling and induration (raised and hard) : as depicted on the arm of the patient in the photograph .
a. 90% of people:
that have a lesion of 10 mm or greater are currently infected with MTB or have been previously exposed to MTB.
b. 100% of people
that have a lesion of 15 mm or greater are currently infected with MTB or have been previously exposed to MTB.
2.False positive tests:
usually manifest themselves as lesser reactions.
These lesser reactions could indicate prior exposure or infection with other mycobacteria or vaccination with BCG.
However, in places were the vaccine is not used, lesser reactions should be regarded as highly suspicious.
False negatives are more rare than false positives but are especially common in AIDS patients as they have an impaired CMI response. Other conditions such as malnutrition, steroids, etc., can rarely result in a false negative reaction.
--------------------------------------------------------------------------------------------------------------
Treatment:
origin, may help to guide treatment. For individuals from areas with low drugresistance,
therapy generally starts with a 2-month course of isoniazid (INH),
rifampin, and pyrazinamide. Multiple drugs are used to avoid resistance.
Directly observed treatment (watching patients take the medication) should be
instituted in all patients in this phase. Subsequently, the patient should receive
a 4-month course of INH and rifampin. Pyridoxine is frequently added to the
regimen. Drug resistance or intolerable side effects may require alternate therapy,
such as with amikacin, ethambutol, or streptomycin. Toxicity for which
patients must be monitored includes hepatitis, hyperuricemia, and thrombocytopenia.
Treatment failure is defined by positive cultures after 3 months or positive
AFB stains after 5 months and should be treated by adding two more drugs.
Latent TB infection should be treated with INH for 9 months, with the goal of
preventing reactivation TB later in life.
----------------------------------------------------------------------------------------------------------
CLINICAL PATHOLOGY:
Summary: A 75-year-old woman dies from massive hemoptysis. Postmortem
examination reveals hilar lymphadenopathy with caseous necrosis and infiltration
and destruction of a large pulmonary artery. Extensive pulmonary consolidation
with other areas of caseous necrosis is noted.
◆ Most likely diagnosis: Pulmonary tuberculosis.
 ◆ Cells likely to be seen on biopsy: Epithelioid cells and Langhans-type
◆ Cells likely to be seen on biopsy: Epithelioid cells and Langhans-typegiant cells typically surround the tuberculous granuloma (tubercle) with
a central area of caseous necrosis.
◆ Usual clinical course: Initial pulmonary involvement with granuloma
formation and later reactivation during times of stress or
immunocompromise.
Figure: Lung specimen depicting pulmonary consolidations
CLINICAL CORRELATION
Worldwide, tuberculosis is the leading cause of death by a single infectious
agent. It is a disease of the socially disadvantaged, the elderly, and the
immunocompromised. This patient probably had been exposed to tuberculosis
sometime earlier and then developed secondary tuberculosis from reactivation
of latent disease or reinfection. The symptoms before presentation with massive
hemoptysis typically would include remittent fever, weight loss, night
sweats, anorexia, general malaise, and weakness.
Hemoptysis occurs in more than 50 percent of patients with secondary
tuberculosis. It is caused by the formation of a cavity between the blood vessels
and the airways. This patient died from blood loss secondary to erosion of
the pulmonary artery. Other causes of death in tuberculosis patients include
massive destruction of the lung parenchyma, constrictive pericarditis from
infection of the pericardial sac, constrictive lung disease from infection of the
pleura, and infection and destruction of other organs and systems, such as the
liver and kidneys.
APPROACH TO TUBERCULOSIS
Objectives
• Describe the etiology of tuberculosis.
• List the pathology and natural history of tuberculosis.
• Know the extrapulmonary manifestations of tuberculosis.
Definitions
Caseous necrosis: Destruction of cells that results in a thick cheese-like
mixture of lipids and proteins.
Delayed-type hypersensitivity: An immune response that takes more than
24 hours to develop and is mediated by T lymphocytes rather than by
antibodies.
Granuloma: A chronic inflammatory lesion made up of an accumulation
of macrophages and giant cells into a discrete, well-formed focus.
PPD test: Purified protein derivatives (PPD) from Mycobacterium tuberculosis
are injected into the dermis. If the body has been exposed to
tuberculosis and immunity has been formed, a hypersensitivity reaction
will occur within 48 to 72 hours, causing a visible wheal.
DISCUSSION
Tuberculosis is caused by members of the M. tuberculosis complex, with the most
 important member being M. tuberculosis itself. Mycobacterium tuberculosis, like
important member being M. tuberculosis itself. Mycobacterium tuberculosis, likeall mycobacteria, is a nonmotile, non–spore-forming aerobic bacterium. It
is covered by a hydrophobic layer made of mycolic acid and other free lipids.
The lipids are acid-fast, meaning that once they are stained by dye, even acid
alcohol cannot remove the stain, and weakly gram-positive. This virtually
impermeable wall, along with other factors, gives M. tuberculosis the ability
to survive phagocytosis by macrophages.
Tuberculosis usually is spread, with rare exceptions, by person-to-person
droplet spread.
figure: CXR PTB
VIDEO ON CXR TB:
A person with active disease can cough up live bacteria in tiny
droplets that can remain airborne in the surrounding currents for several hours.
Within this time, unsuspecting persons can breathe in the droplets, bringing the
bacteria into their lungs. In an immunocompetent person with no previous
exposure to tuberculosis, these invaders quickly are engulfed by the alveolar
 macrophages and carried to the hilar lymph nodes. This is the beginning of
macrophages and carried to the hilar lymph nodes. This is the beginning ofprimary tuberculosis, and it usually takes place in the middle or lower lobes
of the lungs. Unsensitized macrophages cannot fight off the infection because
M. tuberculosis inhibits the acidification of the macrophage lysosomes, not only
surviving phagocytosis but also replicating and destroying the macrophages. The
bacteria then can infect other macrophages or travel through the blood or lymph
to other organs and tissues. During this time, infected persons may experience Figure: CT scan THORAX
what they think is a flu-like illness or may be asymptomatic.
Within 2 to 3 weeks, a hypersensitivity immune response develops. The
formation of this response correlates with the PPD becoming positive.
Through a class II major histocompatibility complex (MHC), the macrophages
present a bacterial peptide to CD4 T cells. These helper cells recognize the
antigen as foreign and produce cytokines such as interferon-γ. The interferon-γ
activates the macrophages, causing them to produce reactive nitrogen intermediates
that are able to kill the mycobacteria and cause the formation of the
epithelioid granulomas. The epithelioid cells can merge, forming the multinucleated
Langhans giant cells. CD8+ T cells cause lysis of the macrophages
through a granule-dependent mechanism and cause death of the mycobacteria.

mechanism, but this does not kill the organisms. This causes progression of the
epithelioid granuloma to a
caseous granuloma.
The initial parenchymal granuloma is referred to as the Ghon focus. The
Ghon focus and the caseated hilar lymph nodes that drain the area are called
the Ghon complex, which subsequently may undergo calcification, becoming
the Ranke complex.
figure: histopathology of Pulmonary tuberculosis:
HISTOPATHOLOGY VIDEO:
Mycobacteria can survive for years within this complex
as latent tuberculosis. A chest x-ray of primary pulmonary tuberculosis typically
shows a single calcified lesion in the parenchymal area.
With secondary pulmonary disease, an exposed person can be reinfected
or there can be reactivation of the latent disease in times of stress. In rare cases,
especially in immunocompromised individuals, primary disease can progress
directly to secondary tuberculosis. Mycobacterium tuberculosis has a high
oxygen requirement during reproduction. Secondary pulmonary tuberculosis
usually occurs in the apex of one or both lungs because of the increased oxygen
content compared with the other areas of the lungs. Because the immune
system already is sensitized to the bacteria, macrophages quickly wall off the
area of infection, resulting in less initial lymph node involvement. The caseous
granuloma forms relatively rapidly, eroding into surrounding airways and
blood vessels. When the granuloma erodes into an airway, the caseous material
drains out of the poorly formed fibrous shell, leaving cavitations. If the
granuloma extends into both airways and blood vessels, it creates a channel for
blood to enter the airway, leading to the classic clinical symptom of hemoptysis.
Drainage of the infectious material into the airways allows for localized
spread through the connected parenchyma. This is the point of the disease at
which a person is most infectious. The airways are full of mycobacteria; it is
estimated that one cough from a person with active tuberculosis can produce
3000 infectious droplets. Proper antibiotic coverage can stop the progression
of the disease, but the body’s attempt to repair the cavitations leads to permanent
damage. The cavitations and areas of caseation are repaired by fibrous
deposits, leaving open pockets or thick scars. These open areas are walled
off from the body and are highly oxygenized, creating a perfect environment
for the fungus Aspergillus to proliferate. A thick ball of fungus can form that
can block the few working airways the patient has left.
In some cases, the lungs may not be the only system involved.
Hematogenous, lymphatic, and direct spread can cause infection in other
systems. In some cases, a single organ may be involved, and dysfunction of
that organ may present before the pulmonary symptoms appear. Table
displays the most common extrapulmonary manifestations of tuberculosis.
In developed countries, tuberculosis had been on the decline for several
years until the emergence of HIV. In the United States, HIV infection is the
greatest risk factor for developing secondary tuberculosis. A normal,
immunocompetent person has a 10 percent lifetime risk of developing secondary
disease, whereas an immunocompromised person has a 10 to 15 percent
yearly risk. A big problem comes from the fact that the presentation of tuberculosis
in an HIV patient is often not the typical presentation. The T-celldependent
mechanism for controlling M. tuberculosis infection is reduced in
these patients.
In HIV patients with moderate immunocompromise, pulmonary tuberculosis
may present as the typical cavitations, but without the lymph node involvement.
The big diagnostic problem comes with severely affected HIV patients
because they may not get cavitations; instead, they may develop pulmonary
and miliary infiltrates. These patients do not have enough T cells to
produce the needed hypersensitivity reaction; therefore, they may not be
PPD-positive. This, combined with the atypical chest x-ray findings, may
delay the diagnosis and treatment of the disease, with devastating results.

-------------------------------------------------------------------------------------------------------------
CLINICAL MICROBIOLOGY:
A 50-year-old man, a recent immigrant from Vietnam, is brought to the emergency room with a cough productive of bloody sputum. He first noticed a cough about 2 months ago, but there was not much sputum. In the past several days his sputum production has increased and become mixed with blood. He reports having lost approximately 15 lb in this time frame as well. He also notes that he's had drenching night sweats 2 or 3 nights a week for the past month. He has a 50-pack-year smoking history but no other medical history. He came to the United States from Vietnam 7 months ago. On examination, he is a thin, frail-appearing male. His vital signs are normal. His head and neck exam is normal. He has no palpable adenopathy in his neck or axilla. His lung exam is notable only for decreased breath sounds diffusely. A chest x-ray shows a cavitary infiltrate of the left upper lobe.
· What type of organism is likely to be seen on Gram stain of a sputum sample?
· What technique of staining is most commonly used to identify this organism?
· What is the histologic characteristic of Langhans' cells?
ANSWERS TO CASE : Mycobacteria
· Likely Gram stain findings of sputum sample: M. tuberculosis appear as colorless ("ghost") cells.
· Most commonly used staining technique for M. tuberculosis: acid-fast staining.
· Histologic characteristics of Langhans' cells: multinucleated giant cells of fused macrophages.
Summary: A 50-year-old Vietnamese man presents with a chronic bloody sputum, weight loss, and a cavitary lesion on chest radiograph, all consistent with tuberculosis.
CLINICAL CORRELATION
Introduction INTRODUCTION TO M.tuberculosis:
It is estimated that M. tuberculosis infects approximately one-third of the world's population. M. tuberculosis is spread from person to person via aerosolized respiratory droplets that travel to the terminal airways. The bacteria are phagocytized by alveolar macrophages but inhibit destruction by the phago-some and proceed to replicate. Circulating macrophages are attracted to the site of infection and create multinucleated giant cells, composed of fused macrophages called Langhans cells. Extrapulmonary sites are infected through the spread of infected macrophages via lymphatic or hematogenous dissemination. Because of the intracellular nature of M. tuberculosis infections, antibody mediated defenses are relatively ineffective. Persons with conditions of reduced cellular immunity, such as AIDS, alcoholism, or drug abuse, or persons living in crowded, close quarters, such as prisoners, are at increased risk for infection. Organisms can remain dormant in granulomas for many years and reactivate following immunosuppression at a later date. At that time the organisms usually infect extrapulmonary sites.
M. avium intracellulare is found in the environment and is an opportunistic pathogen that causes disease in AIDS patients. Disease can range from pneumonia to gastroenteritis to disseminated disease.
M. kansasii can clinically mimic pulmonary tuberculosis, but it is most often seen in middle-aged men with prior lung damage such as silicosis or asbestosis. M. leprae is acquired by contact with the nine-banded armadillo. Most infections are seen in the southern United States including Texas and Louisiana. Thought to be lepers (skin lesions and deformation of the features of the face), these patients were contained in sanitariums and left to die. Infection can be either of the lepromatous or tuberculous type. Most infections caused by rapidly growing Mycobacteria are chronic wound infections, because this organism is found in the soil.
Approach to Suspected Mycobacterial Infection
Definitions
· Langhans cells: Multinucleated giant cells composed of fused macrophages.
· Granuloma: Chronic inflammatory response to either Mycobacterium or fungi, composed of macrophages and multinucleated giant cells.
· PPD: Purified protein derivative, prepared from Mycobacterium tuberculosis antigens inoculated intradermally and a positive reaction is indicative of exposure to M. tuberculosis.
Objectives
1. Know the structure and physiology of Mycobacteria.
2. Know the reservoirs, transmission, and diseases caused by Mycobacteria.
3. Know the mechanisms of host defenses and treatments for Mycobacterial diseases.
Discussion
Characteristics of Mycobacteria Species

Mycobacterium are small rod-shaped bacilli that stain as ghost cells with Gram stain, but because of the presence of mycolic acids in their cell wall stain with an "acid-fast stain" such as Kinyon or Ziehl-Neelsen. This complex, lipid-rich cell wall also makes the organisms resistant to many commonly used laboratory stains and is responsible for the resistance of this organism to many common detergents and antibiotics.
Figure: Microscopy/ZN staining/Acid fast staining

{kind=link}

figure: showing the colony character of M.tuberculosis

In general, Mycobacterium species are slow-growing organisms, with a generation time of 15¾20 hours, compared to about 1 hour for most bacteria. Mycobacterium can be divided into groups as characterized by Runyon, based on their growth characteristics, particularly pigment production. The photo-chromogens, which are pigmented only in the presence of light, include M. kansasii, as well as other saprophytic Mycobacteria. The scotochromogens, which are pigmented even without the presence of light, include M. szulgai, as well as the nonpathogenic M. gordonae, which has an orange pigment. The nonchromogens are not pigmented in the light or dark including M. avium-intracellulare, as well as M. haemophilum. The fourth runyon group is composed of the rapidly growing Mycobacteria such as M. fortuitum, M. chelonae, and M. abscessus. The M. tuberculosis complex includes M. tuberculosis, M. africanum, M. ulcerans, and M. bovis, as well as other rarely identified Mycobacterium. These colonies appear buff or tan color and are dry when growing on Lowenstein-Jensen agar. M. leprae is not considered in that classification because it cannot be cultured in the laboratory.
 One of the virulence factors of M. tuberculosis is cord factor. This can be visualized microscopically as organisms grown in broth culture will demonstrate a ropelike pattern indicating cording. The rapid growing Mycobacterium include M. fortuitum complex, M. chelonae complex, and M. abscessus, as well as other uncommonly isolated nonpathogenic Mycobacteria. These organisms by definition will grow within seven days of subculture onto routine microbiological media such as a blood agar plate
One of the virulence factors of M. tuberculosis is cord factor. This can be visualized microscopically as organisms grown in broth culture will demonstrate a ropelike pattern indicating cording. The rapid growing Mycobacterium include M. fortuitum complex, M. chelonae complex, and M. abscessus, as well as other uncommonly isolated nonpathogenic Mycobacteria. These organisms by definition will grow within seven days of subculture onto routine microbiological media such as a blood agar plate figure: depicting the Lowenstein Jensen culture media for M.tuberculosis
IMMUNOLOGIC -PATHOGENESIS OF TUBERCULOSIS:
The Disease Tuberculosis:
TB infection means that MTB is in the body, but the immune system is keeping the bacteria under control. The immune system does this by producing macrophages that surround the tubercle bacilli. The cells form a hard shell that keeps the bacilli contained and under control. Most people with TB infection have a positive reaction to the tuberculin skin test. People who have TB infection but not TB disease are NOT infectious, i.e., they cannot spread the infection to other people. These people usually have a normal chest x-ray. TB infection is not considered a case of TB disease. Major similarities and differences between TB infection and TB disease are given in the table below.
Tuberculosis: Infection vs Disease
| TB Infection | TB disease in lungs |
| MTB present | MTB present |
| Tuberculin skin test positive | Tuberculin skin test positive |
| Chest X-ray normal | Chest X-ray usually reveals lesion |
| Sputum smears and cultures negative | Sputum smears and cultures positive |
| No symptoms | Symptoms such as cough, fever, weight loss |
| Not infectious | Often infectious before treatment |
| Not defined as a case of TB | Defined as a case of TB |
• Close contact with large populations of people, i.e., schools, nursing homes, dormitories, prisons, etc.
• Poor nutrition
• iv drug use
• Alcoholism
• HIV infection is the #1 predisposing factor for MTB infection. 10 percent of all HIV-positive individuals harbor MTB. This is 400-times the rate associated with the general public
Only 3-4% of infected individuals will develop active disease upon initial infection, 5-10% within one year. These percentages are much higher if the individual is HIV+.
Stages of the Disease
The following stages that will be explained are for a MTB - sensitive host. It should be realized that, as stated previously, only a small percent of MTB infections progress to disease and even a smaller percent progress all the way to stage 5. Usually the host will control the infection at some point.
Disease progression depends on:
• Strain of MTB
• Prior exposure
• Vaccination
• Infectious dose
• Immune status of the host
Stage 1
Droplet nuclei are inhaled. One droplet nuclei contains no more than 3 bacilli. Droplet nuclei are so small that they can remain air-borne for extended periods of time. The most effective (infective) droplet nuclei tend to have a diameter of 5 micrometers. Droplet nuclei are generated by during talking coughing and sneezing. Coughing generates about 3000 droplet nuclei. Talking for 5 minutes generates 3000 droplet nuclei but singing generates 3000 droplet nuclei in one minute. Sneezing generates the most droplet nuclei by far, which can spread to individuals up to 10 feet away.

Spread of droplet nuclei from one individual to another. CDC. After droplet nuclei are inhaled, the bacteria are nonspecifically taken up by alveolar macrophages. However, the macrophages are not activated and are unable to destroy the intracellular organisms.

Tuberculosis begins when droplet nuclei reach the alveoli. When a person inhales air that contains droplets most of the larger droplets become lodged in the upper respiratory tract (the nose and throat), where infection is unlikely to develop. However, the smaller droplet nuclei may reach the small air sacs of the lung (the alveoli), where infection begins.
Stage 2
Begins 7-21 days after initial infection. MTB multiplies virtually unrestricted within unactivated macrophages until the macrophages burst. Other macrophages begin to extravasate from peripheral blood. These macrophages also phagocytose MTB, but they are also unactivated and hence can not destroy the bacteria.
Stage 3
At this stage lymphocytes begin to infiltrate. The lymphocytes, specifically T-cells, recognize processed and presented MTB antigen in context of MHC molecules. This results in T-cell activation and the liberation of cytokines including gamma interferon (IFN). The liberation of IFN causes in the activation of macrophages. These activated macrophages are now capable of destroying MTB.
It is at this stage that the individual becomes tuberculin-positive. This positive tuberculin reaction is the result of the host developing a vigorous cell mediated immune (CMI) response. A CMI response must be mounted to control an MTB infection. An antibody mediated immune (AMI) will not aid in the control of a MTB infection because MTB is intracellular and if extracellular, it is resistant to complement killing due to the high lipid concentration in its cell wall.
Although a CMI response is necessary to control an MTB infection, it is also responsible for much of the pathology associated with tuberculosis. Activated macrophages may release lytic enzymes and reactive intermediates that facilitate the development of immune pathology. Activated macrophages and T-cells also secrete cytokines that may also play a role in the development of immune pathology, including Interleukin 1 ( IL-l), tumor necrosis factor (TNF), and gamma IFN.
It is also at this stage that tubercle formation begins. The center of the tubercle is characterized by "caseation necrosis", meaning it takes on a semi-solid or "cheesy" consistency. MTB cannot multiply within these tubercles because of the low pH and anoxic environment. MTB can, however, persist within these tubercles for extended periods.
Stage 4
Although many activated macrophages can be found surrounding the tubercles, many other macrophages present remain unactivated or poorly activated. MTB uses these macrophages to replicate, and hence, the tubercle grows.
The growing tubercle may invade a bronchus. If this happens, MTB infection can spread to other parts of the lung. Similarly the tubercle may invade an artery or other blood supply line. The hematogenous spread of MTB may result in extrapulmonary tuberculosis otherwise known as milliary tuberculosis. The name "milliary" is derived from the fact that metastasizing tubercles are about the same size as a millet seed, a grain commonly grown in Africa.
The secondary lesions caused by milliary TB can occur at almost any anatomical location, but usually involve the genitourinary system, bones, joints, lymph nodes and peritoneum. These lesions are of two types:
1. Exudative lesions result from the accumulation of PMN's around MTB. Here the bacteria replicate with virtually no resistance. This situation gives rise to the formation of a "soft tubercle".
2. Productive or granulomatous lesions occur when the host becomes hypersensitive to tuberculoproteins. This situation gives rise to the formation of a "hard tubercle".
Stage 5
For unknown reasons, the caseous centers of the tubercles liquefy. This liquid is very conducive to MTB growth, and the organism begins to rapidly multiply extracellularly. After time, the large antigen load causes the walls of nearby bronchi to become necrotic and rupture. This results in cavity formation. This also allows MTB to spill into other airways and rapidly spread to other parts of the lung.
As stated previously, only a very small percent of MTB infections result in disease, and even a smaller percentage of MTB infections progress to an advanced stage. Usually the host will begin to control the infection at some point. When the primary lesion heals, it becomes fibrous and calcifies. When this happens the lesion is referred to as the Ghon complex. Depending on the size and severity, the Ghon complex may never subside. Typically, the Ghon complex is readily visible upon chest X-ray.
Small metastatic foci containing low numbers of MTB may also calcify. However, in many cases these foci will contain viable organisms. These foci are referred to Simon foci. The Simon foci are also visible upon chest X-ray and are often the site of disease reactivation.
Virulence Mechanisms and Virulence Factors
The virulence of Mycobacterium tuberculosis is extraordinarily complicated and multifaceted. Although the organism apparently does not produce any toxins, it possesses a huge repertoire of structural and physiological properties that have been recognized for their contribution to bacterial virulence and to pathology of tuberculosis. Some of the general properties of Mycobacterium tuberculosis that render it virulent are discussed below.
Some general properties of Mycobacterium tuberculosis that contribute to its virulence.
Special mechanisms for cell entry. The tubercle bacillus can bind directly to mannose receptors on macrophages via the cell wall-associated mannosylated glycolipid, LAM, or indirectly via certain complement receptors or Fc receptors.
Intracellular growth. MTB can grow intracellularly. This is an effective means of evading the immune system. In particular, antibodies and complement are ineffective. Once MTB is phagocytosed, it can inhibit phagosome-lysosome fusion. The bacterium secretes a protein that modifies the phagosome membrane. It may remain in the phagosome or escape from the phagosome, in either case finding a protected environment for growth in the macrophage.
Detoxification of oxygen radicals. MTB interferes with the toxic effects of reactive oxygen intermediates produced in the process of phagocytosis by three mechanisms:
1. Compounds including glycolipids, sulfatides and LAM down regulate the oxidative cytotoxic mechanism.
2. Macrophage uptake via complement receptors may bypass the activation of a respiratory burst.
3. The oxidative burst may be counteracted by the production of catalase and superoxide dismutase enzymes.
Antigen 85 complex. This complex is composed of a group of proteins secreted by MTB that are known to bind fibronectin. These proteins may aid in walling off the bacteria from the immune system and may facilitate tubercle formation.
Slow generation time. Because of MTB's slow generation time, the immune system may not readily recognize the bacteria or may not be triggered sufficiently to eliminate them. Many other chronic disease are caused by bacteria with slow generation times, for example, slow-growing M. leprae causes leprosy, Treponema pallidum causes syphilis, and Borrelia burgdorferi causes Lyme disease.
High lipid concentration in cell wall. This accounts for impermeability and resistance to antimicrobial agents, resistance to killing by acidic and alkaline compounds in both the intracellular and extracellular environment, and resistance to osmotic lysis via complement deposition and attack by lysozyme.
Cord factor. Cord factor (trehalose 6, 6' dimycolate) is a glycolipid found in the cell walls of MTB, which causes the cells to grow in serpentine cords. It is primarily associated with virulent strains of MTB. It is known to be toxic to mammalian cells and to be an inhibitor of PMN migration. Its exact role in MTB virulence is unclear, although it has been shown to induce granulomatous reactions identical to those seen in TB
Clinical Identification and Diagnosis of Tuberculosis:
The diagnosis of tuberculosis requires detection of acid-fast bacilli in sputum via the Ziehl-Neelsen method as previously described.
The organisms must then be cultured from sputum. First, the sputum sample is treated with NaOH. This kills other contaminating bacteria but does not kill the MTB present because cells are resistant to alkaline compounds by virtue of their lipid layer.
The media used for growth of MTB and the the resulting colony morphology have been described previously. However, methods of culturing can take 4-6 weeks to yield visible colonies. As a result, another method is commonly used call the BACTEC System. The media used in the BACTEC system contains radio-labeled palmitate as the sole carbon source. As MTB multiplies, it breaks down the palmitate and liberates radio-labeled CO2. Using the BACTEC system, MTB growth can be detected in 9-16 days vs 4-6 weeks using conventional media.
Skin Testing is performed as the tuberculin or Mantoux test. PPD (purified protein derivative) is employed as the test antigen in the Mantoux test. PPD is generated by boiling a culture of MTB, specifically Old Tuberculin (OT). 5 TU (tuberculin units), which equals 0.000lmg of PPD, in a 0.1 ml volume is intracutaneously injected in the forearm. The test is read within 48-72 hours.
Administering the Mantoux test. CDC.
The test is considered positive if the diameter of the resulting lesion is 10 mm or greater. The lesion is characterized by erythema (redness) and swelling and induration (raised and hard). 90% of people that have a lesion of 10 mm or greater are currently infected with MTB or have been previously exposed to MTB. 100% of people that have a lesion of 15 mm or greater are currently infected with MTB or have been previously exposed to MTB.
False positive tests usually manifest themselves as lesser reactions. These lesser reactions could indicate prior exposure or infection with other mycobacteria or vaccination with BCG. However, in places were the vaccine is not used, lesser reactions should be regarded as highly suspicious.
False negatives are more rare than false positives but are especially common in AIDS patients as they have an impaired CMI response. Other conditions such as malnutrition, steroids, etc., can rarely result in a false negative reaction.
Diagnosis:
Diagnosis of tuberculosis is initially made based on a history (exposure to patient with tuberculosis, immigration, a stay in a jail or homeless shelter) and physical exam in patients with a productive cough, night sweats, and fever. A positive PPD test would indicate exposure to M. tuberculosis and warrant further testing with chest x-ray. Patients with the characteristic upper lobe cavitary lesion would have sputum collected and cultured for Mycobacterium.
A fluorescent, direct smear, of the respiratory specimen after decontamination to remove bacterial flora is reported within 24 hours of receipt of the respiratory specimen in the laboratory. Several first early morning deep cough specimens should be collected. Growth of M. tuberculosis on Lowenstein-Jensen (LJ) agar can take 3¾8 weeks because of the slow dividing time of the organism; however, with the use of broth medium growth time has been decreased to as short as 1 week. Newly designed automated broth systems read bottles for growth based on CO2 production of the organisms on a daily basis for up to eight weeks. Bottles which are determined to be positive are stained by Kinyoun stain to visualize the presence of Mycobacteria. Positive bottles can be tested directly for M. tuberculosis, M. kansasii, M. avium-intracellulare, or M. gordonae using DNA probes. Other Mycobacteria species are identified either by routine biochemical tests, which require several weeks, or by high-pressure liquid chromatography, which can speciate Mycobacterium based on mycolic acids extracted from their cell surface. Optimal growth temperature for Mycobacterium species is 35°C (95°F); however, the Mycobacterium that infect the skin such as M. haemophilum grow best at lower temperatures, and organisms such as M. szulgai prefer 42°C (107.6°F). Growth on solid media is also enhanced in the presence of 5¾10% CO2.
Treatment and Prevention:
Prophylaxis for tuberculosis consists of oral isoniazid for 6¾9 months and is given to all patients with a recent conversion of their PPD to positive and a negative chest x-ray. Treatment for tuberculosis based on culture of M. tuberculosis from any patient specimen is initially (first 2 months) with a multiagent regimen based on likely resistance patterns; one such combination is isoniazid, rifampin, ethambutol, and pyrazinamide. Once the results indicate susceptibility to all of the four firstline drugs, treatment can continue with two drugs (usually isoniazid and rifampin) for the remaining 4¾6 months. Because of the interaction of rifampin with other drugs, particularly HIV drugs and antifungals, this therapy may need to be individualized.
Prevention of tuberculosis besides prophylactic isoniazid includes isolation of patients in the hospital to prevent spread. Patients with a positive acid-fast smear must remain in isolation until a diagnosis of tuberculosis is ruled out, until they leave the hospital, or following several weeks of appropriate anti-tuberculous therapy with obvious clinical improvement. All known close contacts (family members) of the index case should have a PPD test to determine if they should be given therapy and/or worked up for disease.
Vaccination with BCG, (an attenuated strain of M. bovis) is not routinely performed in the United States because of the comparatively low incidence of tuberculosis. Protection from tuberculosis is not 100 percent with the vaccine and can confuse the results of the PPD for screening of recent converters.
Treatment of the other atypical Mycobacteria varies based on the species. M. avium-intracellulare is usually treated with clarithromycin or azithromycin and ethambutol plus or minus amikacin. Current treatment for leprosy is dapsone and rifampin for at least 6 months.
-------------------------------------------------------------------------------------------------------------
author: Abhishek soni (medico)
college: Index medical college and research center, Indore, M.P., India